minor confidentiality & consent laws + mandated reporting
Important: This page summarizes Maryland law only. Many states have similar concepts regarding minor consent, confidentiality, and mandated reporting, but the details vary significantly from state to state. If you live outside Maryland, consult your state's laws or a qualified attorney.
before you begin:
consent - who can make the decision?
confidentiality - who can know?
mandated reporting - what must be reported despite confidentiality?
The same situation may involve all three concepts. For example, a teenager may be able to consent to receiving therapy, keep some information confidential, and still be subject to reporting requirements in certain circumstances.
question
quick answer
Q: Can a minor start outpatient therapy without parental permission?
A: Yes, age 12+ only
Q: Can a minor consent to psychiatric medication without parental permission?
A: Yes, age 16+ only
Q: Can a minor get birth control without parental permission?
A: Yes, minors may consent on their own
Q: Can a minor get STI testing or treatment without parental permission?
A: Yes, minors may consent on their own
Q: Can a minor receive pregnancy-related care without parental permission?
A: Yes, minors may consent on their own
Q: Can a minor obtain an abortion without parental involvement?
A: Yes, but in most cases, parental notification is required
Q: Can parents automatically access all therapy information?
A: No, some information may remain confidential
Q: Are there limits to confidentiality?
A: Yes, safety concerns and reporting laws create exceptions
Q: What if parents are divorced?
A: Legal custody determines decision-making rights
minor consent
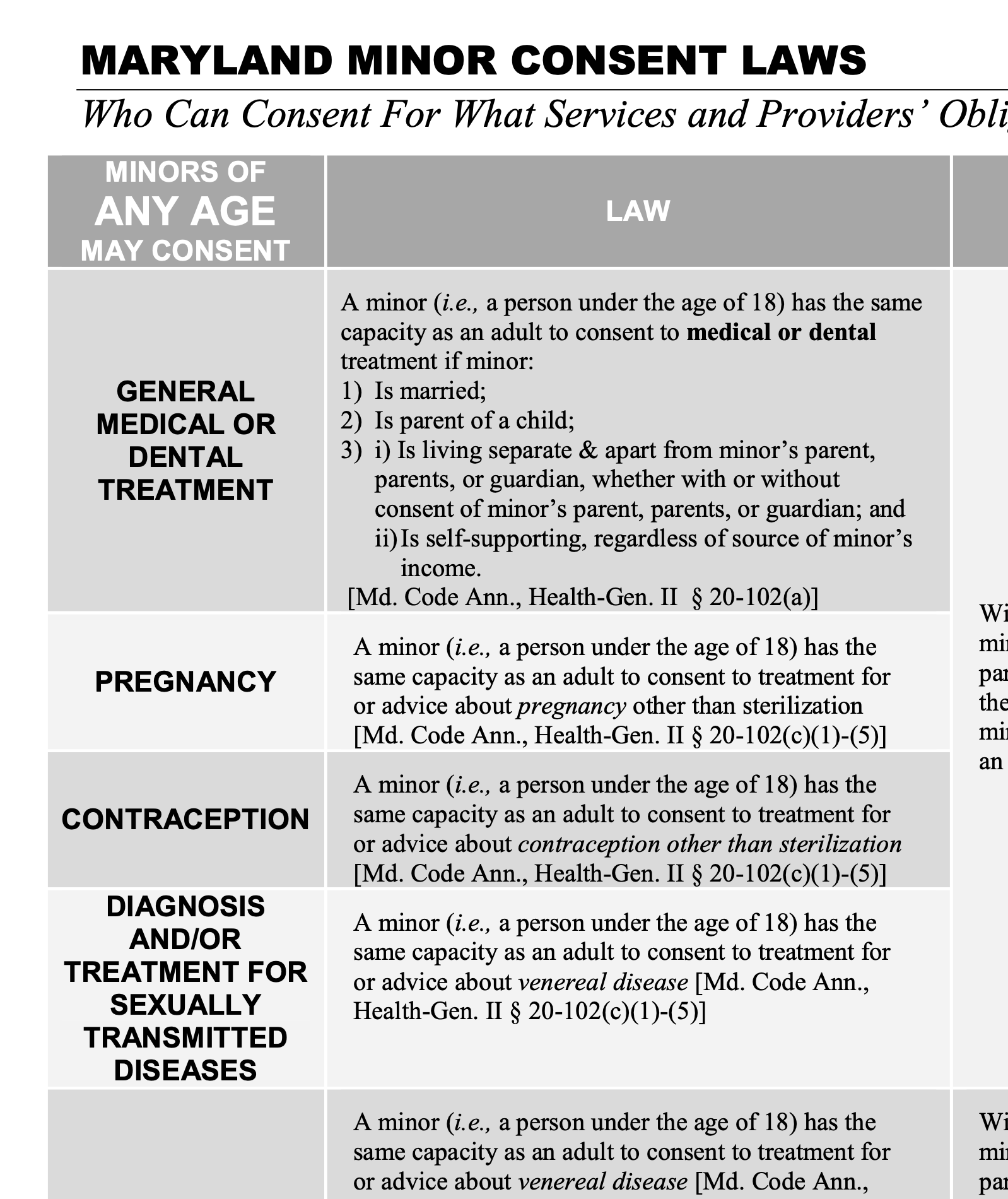
Most healthcare decisions for minors are made by parents or legal guardians. Maryland law allows minors to independently consent to certain types of healthcare, including outpatient mental health treatment, contraception, STI care, pregnancy-related care, and several other services.
-
Yes. In Maryland, minors age 12 and older who are determined to be mature enough to provide informed consent may consent to outpatient mental health treatment without parental permission.
-
Not necessarily. Maryland law gives many minors age 12 and older the ability to consent to outpatient mental health treatment. Practical issues such as transportation, payment, custody arrangements, and clinical considerations may affect whether treatment can continue, but a parent's disagreement does not automatically cancel treatment.
-
Only if they are age 16 or older. Maryland allows minors age 12 and older to consent to outpatient therapy, but minors under age 16 generally cannot independently consent to prescription psychiatric medication.
-
Yes. Minors may consent to contraception without parental permission. This includes most forms of birth control, but not sterilization.
-
Yes. Minors may consent to testing, treatment, and medical advice related to sexually transmitted infections without parental permission.
-
Yes. Minors may consent to pregnancy-related medical care and counseling without parental permission.
-
Maryland generally requires parental notification before an abortion for an unmarried minor, but there are several exceptions. A physician may proceed without notification under certain circumstances, including concerns about abuse, maturity of the minor, or the minor's best interests.
-
Married minors generally have the same ability as adults to consent to their own medical care.
-
Minors who are parents generally have the same ability as adults to consent to their own medical care.
-
A minor who is living apart from their parents and is financially self-supporting may be able to consent to their own healthcare. This provision was primarily intended to ensure access to care for homeless and runaway youth.
confidentiality
Confidentiality determines who can access information about healthcare. Consent and confidentiality are related, but they are not the same thing. A minor may be able to consent to treatment, keep some information private, and still have certain information shared in specific circumstances.
-
Not necessarily. Consent and confidentiality are related, but they are not the same thing. A minor may be able to consent to treatment while still allowing some information to be shared with parents, and some situations may require disclosure regardless of consent.
-
Yes. Therapists frequently communicate with parents about treatment goals, progress, safety concerns, and family issues. However, specific details discussed in therapy may remain private.
-
Sometimes. In Maryland, when a minor is legally allowed to consent to treatment, the minor may also have rights regarding access to related records. Parents do not automatically have unlimited access to every therapy record simply because they are the parent. Access can depend on who consented to treatment, the type of treatment involved, the minor's age, Maryland confidentiality laws, and HIPAA.
-
Personal thoughts, feelings, relationships, identity exploration, and other topics commonly discussed in therapy are often kept confidential. Privacy helps adolescents speak honestly and develop trust in treatment.
-
Therapists often share information needed to support treatment, such as attendance problems, significant safety concerns, worsening symptoms, treatment recommendations, medication concerns, family dynamics affecting treatment, and ways parents can help. The goal is usually to provide parents with useful information without sharing every detail discussed in therapy.
-
Confidentiality helps treatment work. Adolescents are often more willing to discuss difficult topics when they know every detail will not automatically be shared. Most therapists aim to balance a teenager's privacy with a parent's need to support their child's safety and wellbeing.
-
Privacy means that a therapist does not automatically share everything discussed in therapy. Secrecy means that information must be hidden from other people.
Most adolescent therapy is built around privacy, not secrecy. Therapists may be limited by confidentiality laws and professional ethics, but parents and teenagers are generally free to talk with one another about whatever they choose.
The goal is not to keep parents out of treatment, but to create enough privacy for honest conversations while still supporting communication, trust, safety, and family involvement.
safety concerns
Confidentiality may be limited when a therapist believes someone is at risk of serious harm. The response depends on the specific situation, the level of risk, the client's age, and other factors. There is no single rule that applies to every situation. There is no list of words that automatically trigger hospitalization, parent notification, or reporting. Therapists evaluate the overall situation, level of risk, and available supports before deciding how to respond.
teen questions
-
Maybe. Therapists consider the severity of the risk, the client's age, available supports, and other factors. If a therapist believes a client is at significant risk of harm, they may involve parents or other supports to help keep the client safe.
-
Not necessarily. Most disclosures of suicidal thoughts do not automatically result in hospitalization. Therapists assess the level of risk and work with clients and families to determine the safest response.
-
Maybe. The answer depends on the severity of the self-harm, the level of medical risk, the client's age, and other circumstances.
-
Usually not. Self-harm alone does not automatically lead to hospitalization. Therapists evaluate the level of risk and whether additional support or intervention is needed.
-
Maybe. Concerns about nutrition, weight loss, purging, medical complications, or other safety risks may require parent involvement, particularly for younger adolescents.
-
Not automatically. However, severe eating disorder symptoms can create serious medical risks. Therapists may recommend medical evaluation or higher levels of care when necessary.
-
Substance use alone does not automatically require parent notification or a mandated report. However, concerns about overdose risk, severe impairment, dangerous situations, medical complications, or other significant safety concerns may lead a therapist to involve parents or other supports. Therapists often encourage open discussion about substance use. Whether information is shared depends on the client's age, safety concerns, and the circumstances involved.
-
In Maryland, consensual sexual activity between adolescents does not automatically require parental notification or a CPS report. Therapists may discuss pregnancy prevention, STI testing, healthy relationships, and safety, but disclosure depends on the circumstances rather than the fact that sexual activity occurred.
-
Usually not. Sexual activity between adolescents does not automatically trigger a report. However, age differences, coercion, exploitation, or concerns about abuse may change the situation.
-
Often yes. Sexual contact between a minor and an adult may raise concerns about abuse, exploitation, trafficking, coercion, or violations of Maryland law. Therapists generally need to assess the ages involved, the nature of the relationship, and whether reporting obligations or safety interventions apply.
-
Not automatically. Reporting depends on factors such as age differences, coercion, exploitation, abuse, and the circumstances involved. Consensual sexual activity between teenagers does not automatically require a report.
-
Not necessarily. The answer depends on the nature of the harm, whether anyone is currently at risk, the client's age, and whether reporting laws apply.
-
Usually. When possible, therapists often discuss concerns and next steps with clients before contacting parents, hospitals, emergency services, or other supports.
-
Yes. Therapists may involve parents, emergency contacts, hospitals, or other supports to address safety concerns even when no mandatory report is required.
-
Not automatically. Therapists generally treat this information the same way they would other information shared in therapy. However, concerns about abuse, exploitation, trafficking, or serious safety risks may require additional action.
-
No. Therapy is not intended to create secrets between teenagers and parents. The goal is to provide enough privacy for honest conversations while still involving parents when necessary to support treatment and safety.
-
Not automatically. Therapists generally consider confidentiality laws, the client's age, safety concerns, and the potential risks and benefits of disclosure before sharing information about identity-related issues.
parent questions
-
Self-harm exists on a spectrum. Some self-harm indicates an immediate risk of serious injury and may require parent involvement. Other self-harm may be addressed within treatment while the therapist works to reduce risk and build coping skills. Therapists consider the severity, frequency, medical risk, suicide risk, age of the client, and the likely impact of disclosure before deciding how to respond.
-
Not every risky behavior requires parent notification. Therapists often balance a teenager's privacy with a parent's need to know important information. The response depends on the client's age, the level of risk, and the circumstances involved.
-
Therapists often encourage honest discussions about substance use. In some situations, maintaining confidentiality may help a teenager stay engaged in treatment and reduce risk. In other situations, parent involvement may be necessary.
-
Maryland law allows minors to independently consent to contraception, STI testing and treatment, and pregnancy-related care. Because of these laws, therapists often approach adolescent sexual health differently than other topics and may not automatically disclose consensual sexual activity to parents.
-
School attendance and academic performance may be discussed in therapy without automatically being disclosed to parents. Therapists often encourage teenagers to address these concerns directly with their families whenever possible.
-
Therapy is not intended to be a secret-keeping relationship, but it is not a surveillance relationship either. Adolescents are often more willing to discuss difficult topics when they know every detail will not automatically be shared. Most therapists aim to balance a teenager's privacy with a parent's ability to support treatment and safety.
-
There is no single rule. Therapists consider the client's age, maturity, safety concerns, treatment goals, family circumstances, and applicable laws when deciding what information should remain private and what information should be shared.
-
Sometimes. Therapists may withhold information when confidentiality laws apply or when disclosure would interfere with treatment without providing a clear safety benefit.
-
Adolescents need some private space to talk honestly about relationships, identity, mental health, family stress, safety concerns, and other sensitive topics. Most therapists balance private conversations with ongoing parent involvement rather than excluding parents from treatment.
HIPAA
The Health Insurance Portability and Accountability Act
-
HIPAA is a federal privacy law that regulates how healthcare information may be used and shared. HIPAA protects medical information, but it does not automatically prevent parents from receiving information about their child's healthcare.
-
HIPAA is a federal privacy law, but access to a minor's healthcare information is also affected by Maryland law, custody arrangements, consent laws, insurance communications, and the type of treatment involved.
-
No. HIPAA does not automatically prevent parents from accessing information about their child's healthcare. Access depends on federal law, Maryland law, custody arrangements, the type of treatment involved, and who consented to the treatment.
-
No. HIPAA generally follows state laws governing minors' rights to consent to care and control access to related records.
-
Often yes. When insurance is not billed, there is generally no claim submitted to an insurance company and no Explanation of Benefits (EOB) generated. However, privacy can still be affected by billing arrangements, payment methods, shared financial accounts, and other circumstances. Paying out of pocket may reduce, but does not guarantee, confidentiality.
insurance & billing
-
Not always. Insurance companies often send Explanation of Benefits (EOB) statements and other claim information to the policyholder. Even when treatment itself is confidential, insurance communications may reveal that healthcare services were provided.
-
An EOB is a statement sent by an insurance company showing how a claim was processed. It is not a bill, but it may contain information about healthcare services that were received.
-
Yes. A minor's legal ability to consent to treatment does not necessarily create a financial obligation for a parent. A parent may decline to pay for treatment that the minor independently consented to receive. As a result, a minor may have a legal right to seek treatment but still face practical barriers related to payment, transportation, scheduling, or insurance.
-
Sometimes. Insurance claims, Explanation of Benefits (EOB) statements, billing records, appointment reminders, patient portals, and payment methods may all affect what information is visible to a parent or policyholder.
mandated reporting
Confidentiality has limits. Sometimes information must be shared because Maryland law requires a report. Other times information may be shared because a therapist believes someone is at risk of serious harm and needs additional support.
Is a safety concern the same thing as a mandated report?
No. Mandated reporting and safety interventions are different. A therapist may contact CPS because the law requires it, or may contact parents, hospitals, or crisis services because someone is at risk. Sometimes both happen, but often only one applies.
-
Mandated reporting laws require certain professionals to report suspected abuse, neglect, exploitation, or serious safety concerns. Therapists, physicians, teachers, social workers, and many other professionals are mandated reporters.
-
Suspected child abuse
Suspected child neglect
Suspected child sexual abuse
Certain vulnerable adult abuse situations
Communicable diseases, serious threats of harm, and specific injuries covered by law — “duty to warn”
-
Consensual sexual activity between teenagers (with important exceptions)
Substance use
Teen dating violence involving a non-caregiver
Adult domestic violence
Adult sexual assault
-
No. Mandated reporting and parental notification are separate issues. A report may be made to Child Protective Services, Adult Protective Services, or another agency without sharing all details with parents.
-
Most reports are reviewed by Child Protective Services (CPS), Adult Protective Services (APS), or law enforcement to determine whether the report meets criteria for investigation. Some reports are screened out. Others result in interviews, requests for information, safety assessments, referrals to services, or formal investigations. A report does not automatically mean someone is charged with a crime or that a child is removed from the home.
-
No. Most reports do not result in removal. A report begins an assessment or investigation; it does not determine the outcome.
-
Usually. When safety allows, therapists often discuss reporting obligations with clients before making a report. However, there may be situations where immediate action is required.
-
Yes. Mandated reporters can face legal or professional consequences for failing to make required reports.
-
Yes. Mandated reporters are generally required to report reasonable suspicion, not prove that abuse or neglect occurred. Determining what happened is the responsibility of the investigating agency.
-
A report may still be required. Mandated reporters are not responsible for determining whether abuse occurred; they are responsible for reporting concerns when required by law.
-
A therapist may still have a legal obligation to report. Reporting requirements generally cannot be waived by the child, parent, or therapist.
-
No. If a report is legally required, a parent's objection does not eliminate the therapist's reporting obligation.
-
Sometimes. Therapists may disclose information in certain situations involving serious and imminent safety concerns, even when a mandatory reporting law does not apply.
-
Not necessarily. Unlike child sexual abuse, past physical abuse disclosed by an adult does not automatically trigger a report in every situation. Reporting obligations often depend on factors such as whether a child is currently at risk, whether the alleged perpetrator still has access to children, and the specific circumstances involved.
CSA reporting
Child sexual abuse reporting is one of the most commonly misunderstood areas of mandated reporting. In Maryland, reporting obligations may still apply even when the abuse occurred years ago or the victim is now an adult. The specific circumstances matter, and reporting obligations can differ from those involving other forms of past abuse.
A report is not the same thing as an investigation, and an investigation is not the same thing as a criminal charge.
-
Often yes. Maryland generally requires reporting even when the victim is now an adult, unless the reporter can independently verify that the abuse has already been reported.
-
The passage of time does not automatically eliminate reporting obligations.
-
Reporting oSometimes. Maryland's reporting requirements for child sexual abuse can still apply even when the victim is now an adult. The key question is often whether the therapist has information suggesting child sexual abuse occurred, not the victim's current age.
-
This may affect how a report is handled, but it does not automatically eliminate reporting obligations.
-
If the reporter can independently verify that a report was previously made, a new report may not be required.
-
The therapist may still have legal reporting obligations.
-
Not necessarily. Reporting obligations vary depending on the circumstances. Even when a report is required, that does not automatically mean police will immediately contact the victim or begin a criminal investigation.
-
Sometimes. Therapists are generally required to report concerns when reporting laws apply, even if some information is missing. The investigating agency determines whether enough information exists to proceed.
-
Partial memories, uncertainty, or incomplete information do not automatically eliminate reporting obligations. Therapists are not responsible for determining whether abuse definitely occurred; they are responsible for understanding when a report may be legally required.
-
A disclosure may still trigger reporting obligations even if it is the first time the abuse has ever been discussed.
-
A client's wishes are important and therapists generally discuss concerns openly whenever possible. However, reporting obligations cannot usually be waived by the client, parent, or therapist when the law requires a report.
-
Reporting obligations may still apply. Agencies determine jurisdiction and which state is responsible for investigating the report.
-
Online sexual exploitation, solicitation, coercion, image sharing, and related conduct may still qualify as reportable abuse depending on the circumstances.
-
Concerns that an alleged perpetrator may currently have access to children can affect how a report is evaluated and why reporting obligations may continue even years after the abuse occurred.
-
Reporting requirements may differ depending on the ages involved, the nature of the conduct, whether coercion was involved, and other circumstances.
-
Exact dates and ages are not always necessary for a therapist to recognize a potential reporting obligation. Investigating agencies are responsible for gathering additional information when needed.
-
Usually, yes. When safety allows, therapists often discuss reporting obligations and next steps with clients before making a report. However, there may be situations where immediate action is necessary.
-
Reporting obligations generally do not depend on who committed the abuse. The same reporting laws apply whether the alleged perpetrator is a parent, relative, caregiver, family friend, teacher, coach, clergy member, or another person.
-
Not all sexual contact between minors is treated the same way. Factors such as age differences, coercion, force, exploitation, developmental differences, and the specific circumstances may affect whether reporting obligations exist.
-
Not always. Childhood sexual abuse and childhood physical abuse may involve different reporting considerations. The therapist must evaluate the specific facts, applicable laws, and whether anyone is currently at risk. Maryland reporting laws may apply differently depending on the type of abuse and the circumstances involved. Reports of childhood sexual abuse may still require action years later, while reports of past physical abuse often focus more heavily on whether any child is currently at risk.
age of consent, statutory rape, & reporting
-
Not automatically. Consensual sexual activity between teenagers does not automatically trigger a CPS report. Therapists consider factors such as age differences, coercion, exploitation, developmental differences, and applicable Maryland law.
-
Not necessarily. Age-of-consent laws and mandated reporting laws are related but not identical. Therapists evaluate the specific circumstances rather than relying solely on a person's age.
-
No. Age-of-consent laws help determine whether sexual activity is legally permitted, but mandated reporting decisions may involve additional factors such as age differences, coercion, force, exploitation, grooming, authority relationships, and whether a child is currently at risk.
-
Often yes. Larger age differences may raise concerns about exploitation, coercion, or abuse. Therapists generally need to evaluate the specific facts and determine whether reporting obligations apply.
-
Not automatically, but therapists generally must carefully assess the situation. The ages involved, the nature of the relationship, and Maryland reporting laws may all affect whether a report is required.
-
A teenager's belief that a relationship is consensual does not automatically eliminate concerns about abuse, exploitation, grooming, trafficking, or statutory offenses. Therapists evaluate the entire situation, not just whether the teenager objected.
-
Maybe. Sexual images involving minors can raise legal and safety concerns even when the images were voluntarily shared. Therapists evaluate the circumstances, the ages involved, and whether anyone is currently at risk.
parents, guardians, & decision-making
Not every adult has the same authority to make healthcare decisions for a minor. Legal custody, court orders, guardianship arrangements, and other legal relationships determine who may consent to treatment.
-
Legal custody, not marital status, determines healthcare decision-making authority. Parents who share legal custody generally share authority to make major healthcare decisions. Parents should review their custody order to determine whether decision-making authority is shared or assigned to one parent.
-
Not always. Some custody orders require joint decision-making for major healthcare decisions, while others give one parent final decision-making authority. The answer depends on the specific custody order.
-
A parent with sole legal custody generally has authority to make healthcare decisions without obtaining permission from the other parent, unless a court order provides otherwise.
-
When parents share legal custody and disagree about treatment, providers may encourage parents to resolve the disagreement directly. In some situations, court involvement may be necessary to determine how decisions will be made.
-
Usually not simply because they are a grandparent. However, grandparents may be able to consent if they have legal guardianship, custody, or another legal authority to make healthcare decisions.
-
Maryland allows certain relatives providing informal kinship care to consent to healthcare when specific legal requirements are met. This helps ensure that children living with relatives can receive necessary medical care even when a parent is unavailable.
-
Sometimes. Foster care cases often involve separate rules that may assign decision-making authority to parents, social services, the court, foster parents, or the minor depending on the circumstances.
-
Healthcare providers may provide emergency treatment without parental consent when delaying treatment would place the minor at substantial risk of serious harm and an authorized decision-maker is not immediately available.
-
A minor who is living separately from their parents and is self-supporting may be able to consent to their own healthcare. This provision was largely intended to address situations involving homeless or runaway youth.
-
A married minor generally has the same capacity as an adult to consent to medical treatment.
-
A minor who is the parent of a child generally has the same capacity as an adult to consent to medical treatment.
-
Often yes, but not always. Access may depend on custody orders, the type of treatment involved, who consented to treatment, and applicable confidentiality laws.
downloads & resources
Lower Age for Consent Took Effect October 1 | Maryland Psychiatric Society
§ 20-104. Consent of minor to treatment of mental disorder - Maryland Code and Court Rules
Maryland Mental Health Available to 12-Year-Olds | Modern Family Law
Legislation - SB0041 - Health – Mental and Emotional Disorders – Consent (Mental Health Access Initiative)
The Maryland Assembly on School Based Health Care (MASBHC) - Webinars & Trainings - “Maryland Minor Consent for Mental Health Care Law Update” September 29, 2021, by the following list of speakers: Delegate Heather Bagnall, District 33 Larry Epp, Ed.D., LCPC. Sheppard Pratt-Gaithersburg and Jill Bohnenkamp, Ph.D., National Center for School Mental Health
Minors & Behavioral Health: Maryland Consent Laws - University of Maryland Medical Center and Maryland Behavioral Health Integration in Pediatric Primary Care
Maryland Minor Consent for Mental Health Care Law Update
MD minor consent laws - American Academy of Pediatrics MD Chapter
Maryland Minor Consent and Confidentiality - National Center for Youth Law
University of Maryland School of Medicine - Minor Consent in School Based Health Centers: Considerations for Implementation
Adolescent & Young Adult Health Care in Maryland - A Guide to Understanding Consent & Confidentiality Laws Abigail English, JD, Center for Adolescent Health & the Law
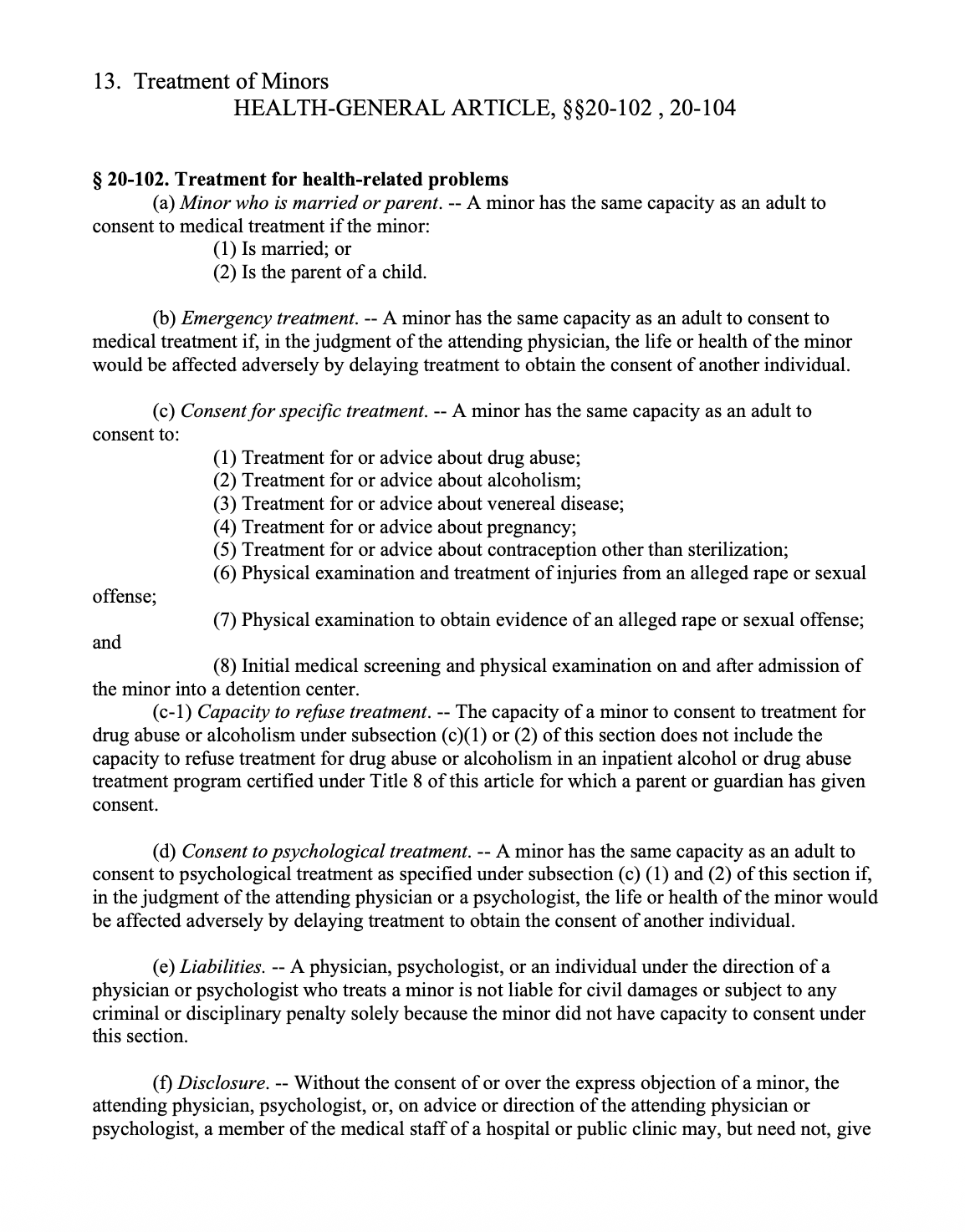
Treatment of Minors HEALTH-GENERAL ARTICLE, §§20-102 , 20-104
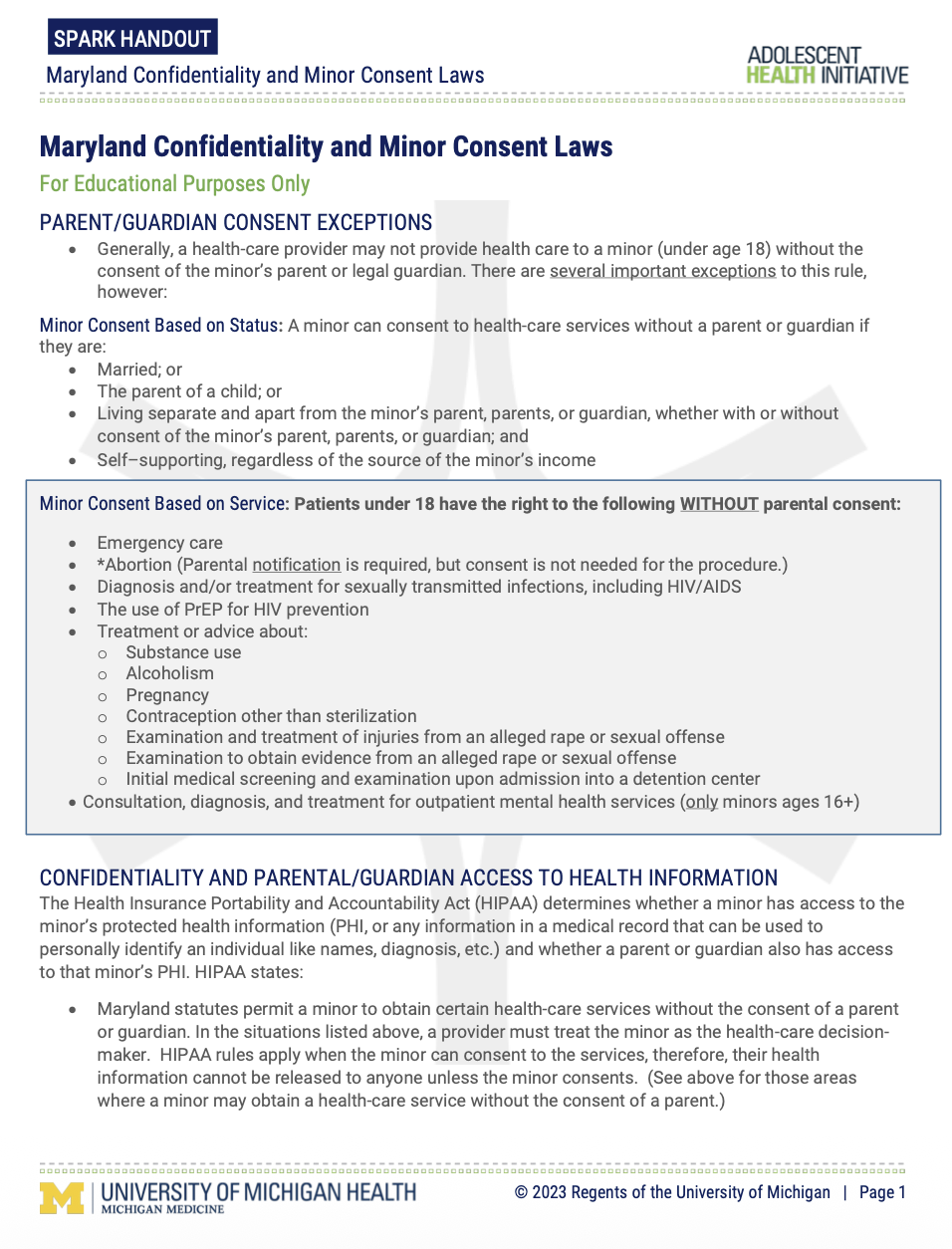
University of Michigan Adolescent Health Initiative - Maryland Confidentiality and Minor Consent Laws

The Network for Public Health Law - Maryland: Laws Regarding Minor Consent to Health Care
The Mental Health Access Initiative (SB 41) : Why was it needed? Larry Epp, Ed.D. Director of Outcomes and Innovation Communities and Families Service Line Sheppard Pratt & Board Member, Licensed Clinical Professional Counselors of Maryland
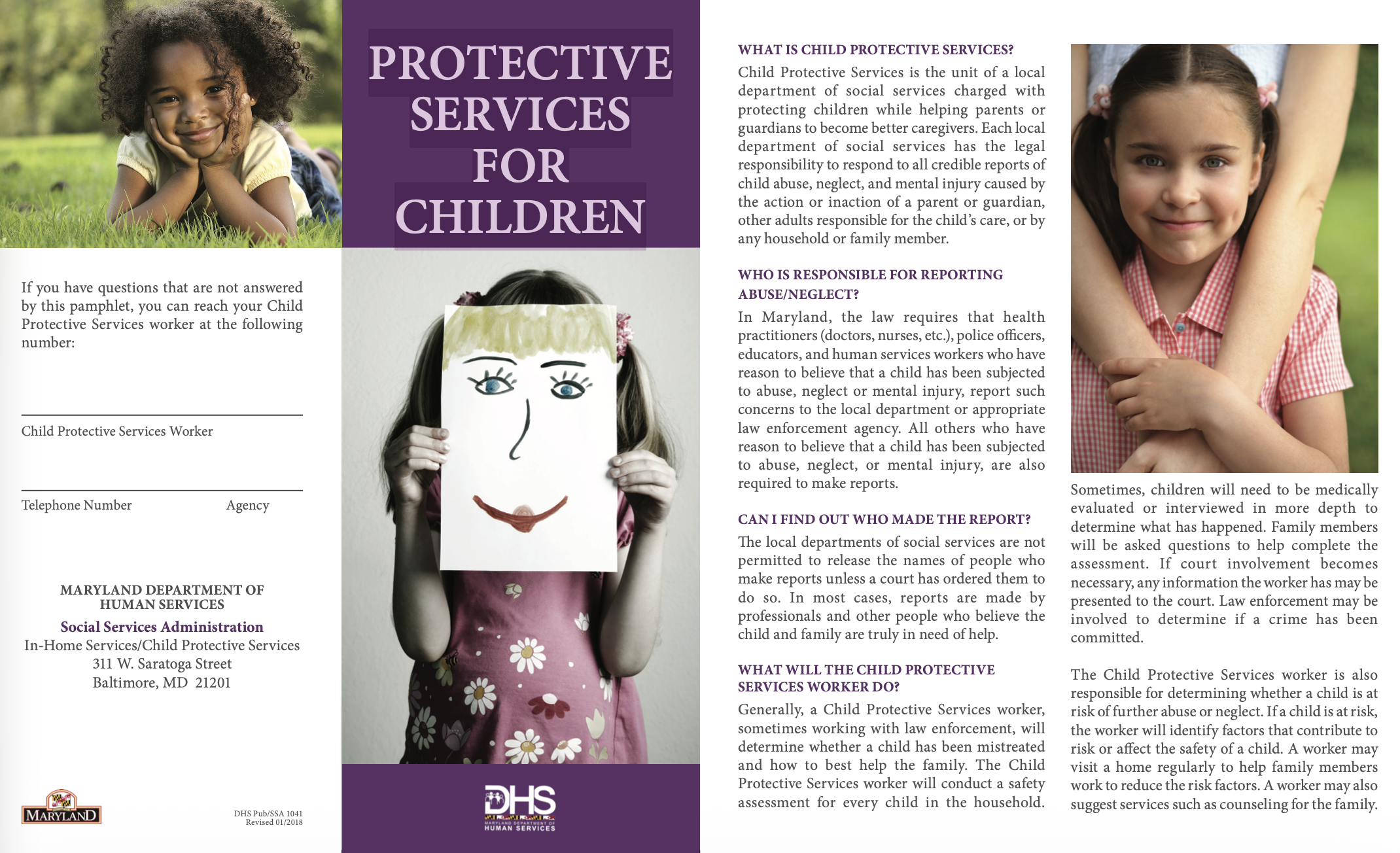
Maryland DHS - Protective Services for Children
Maryland Healthcare Coalition Against Domestic Violence - Confidentiality & Mandated Reporting Requirements in Maryland